Contrast Agent Evaluation - Imaging in Medicine (2013) Volume 5, Issue 2
Tc-tilmanocept for lymphoscintigraphy
Christopher A Puleo1, Claudia Berman1,2,3,4, Jaime L Montilla-Soler2,3,4, Jonathan S Zager1,3,5 & Vernon K Sondak*1,3,51Department of Cutaneous Oncology, Moffitt Cancer Center, Tampa, FL, USA
2Department of Diagnostic Radiology, Moffitt Cancer Center, Tampa, FL, USA
3Department of Oncologic Sciences, University of South Florida Morsani College of Medicine, Tampa, FL, USA
4Department of Radiology, University of South Florida Morsani College of Medicine, Tampa, FL, USA
5Department of Surgery, University of South Florida Morsani College of Medicine, Tampa, FL, USA
- Corresponding Author:
- Vernon K
Sondak
Department of Cutaneous Oncology
Moffitt Cancer Center, Tampa, FL, USA
Tel: +1 813 745 8788
Fax: +1 813 745 7211
E-mail: vernon.sondak@moffitt.org
Abstract
Keywords
breast cancer ▪ intraoperative lymphatic mapping ▪ lymphoscintigraphy ▪ melanoma ▪ sentinel lymph node biopsy
Lymphoscintigraphy & intraoperative lymphatic mapping for sentinel lymph node biopsy in breast cancer & melanoma
The concept of sentinel node biopsy is based on the anatomic observation that lymphatic flow proceeds in an orderly fashion from the site of a primary tumor (at least for tumors on the skin or in the breast and probably for visceral tumors as well), to one or a few primary draining lymph nodes, which may or may not be within a regional node basin [1]. The histologic status of these ‘sentinel’ lymph nodes is highly predictive of the remaining lymph nodes; in general, less than 5% of patients with melanoma or breast cancer whose sentinel lymph nodes are negative for malignancy ever manifest evidence of regional nodal metastasis [2]. Furthermore, by removing only one or a few lymph nodes, morbidity is dramatically reduced compared with a full regional lymphadenectomy and enhanced techniques of histologic assessment can be used to detect even very small metastatic deposits, far below the resolution of any available imaging technique.
But while lymphatic flow is orderly, it is not necessarily predictable in a specific individual or tumor. Time-honored concepts of lymphatic anatomy such as Sappey’s lines, which divide the trunk into four quadrants that ostensibly drain to the nearest regional node basin, have proven insufficiently accurate for clinical use, and the rich and varied lymphatic drainage of the head and neck provides a particular challenge [3,4]. Lymphatic mapping utilizing preoperative radionuclide lymphoscintigraphy with 99mTc-labeled colloidal suspensions, supplemented by intraoperative injections of vital blue dyes, have allowed surgeons to identify all regional nodal basins at risk and also find ‘in-transit’ nodes when they exist outside the anatomic confines of standard basins [5]. Sentinel node biopsy is a minimally invasive surgical technique that has virtually eliminated elective node dissection from the management of melanoma and breast cancer. By providing superior staging with decreased morbidity, the use of sentinel node biopsy has helped to revolutionize the staging and treatment of melanoma and breast cancer in the last two decades, and will probably have a role to play in staging other cutaneous malignancies (e.g., Merkel cell carcinoma) and potentially many noncutaneous tumors (e.g., squamous cell carcinoma of the upper aerodigestive tract) where complete lymphadenectomy is currently the standard staging approach. The authors’ intent is to review the available literature on a newly US FDA-approved agent for intraoperative lymphatic mapping, 99mTc-tilmanocept (Lymphoseek), without speculating on data or topics that are currently not substantiated.
Overview of the market
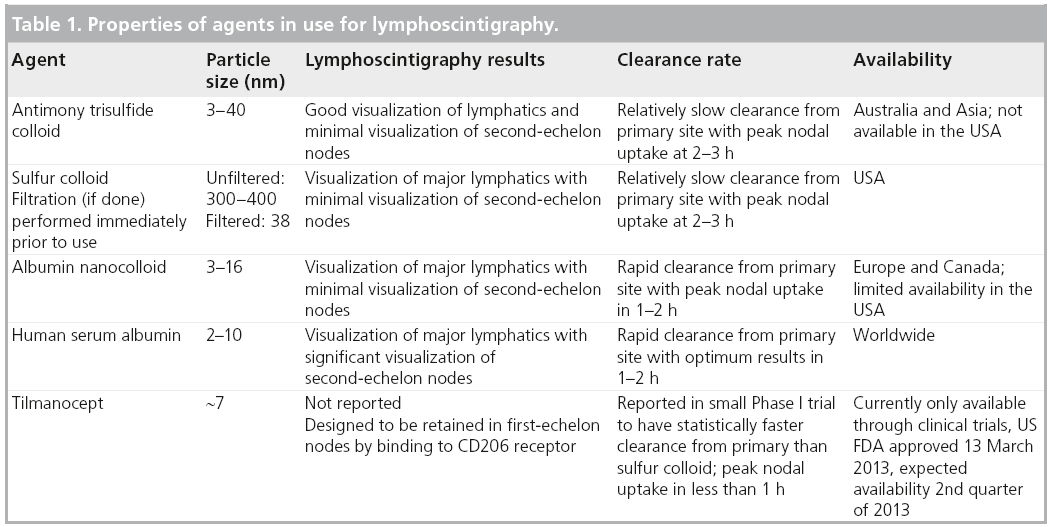
At the present time, sentinel node biopsy is widely used in the surgical management of clinically localized breast cancer, cutaneous melanoma and some other cutaneous malignancies (particularly Merkel cell carcinoma). Worldwide, there were an estimated 1.38 million cases of breast cancer diagnosed in 2008 (the last year for which global data are available), with an estimated incidence rate of 66.4 per 100,000 women in developed countries [6]. Melanoma is slightly less common worldwide (8.6–9.5 per 100,000 people in developed countries), but still a significant problem with a rising incidence rate in most of the world. The majority of patients with either breast cancer or melanoma present with clinically localized disease, and are therefore, potential candidates for lymphatic mapping and sentinel node biopsy. In many hospitals in the USA, preoperative lymphoscintigraphy for sentinel node localization is the most commonly performed nuclear medicine imaging study. Almost all sentinel node biopsy procedures for breast cancer and melanoma are performed using a radiolabeled tracer, but there is no consensus on which tracer is best (Table 1). Accordingly, the potential worldwide market for an agent that provides superior performance (e.g., faster clearance from the injection site, quicker uptake in the sentinel nodes, and less spread to second echelon nodes in the regional nodal basin) or offers financial advantages compared with currently available tracers would be substantial. In the future, it is possible that lymphoscintigraphy and sentinel node biopsy will be used more frequently in selected noncutaneous malignancies (particularly head and neck and gastrointestinal malignancies), which would obviously represent a substantial and dramatic increase in the potential market for radiolabeled lymphatic mapping agents.
Introduction to the compound
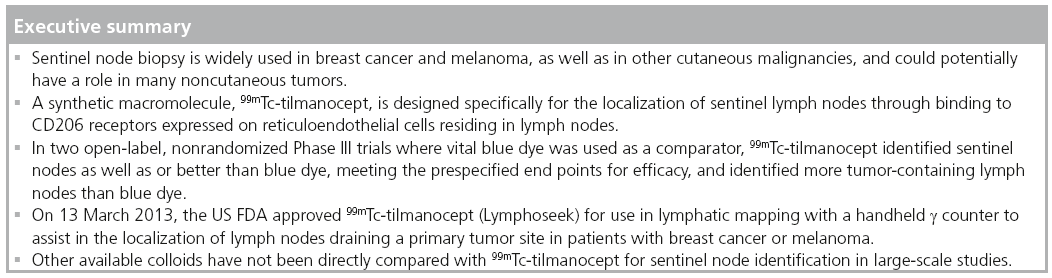
99mTc-tilmanocept (Lymphoseek™; Navidea Biopharmaceuticals Inc., OH, USA), is a synthetic macromolecule designed with multiple mannose moieties intended to allow specific multivalent binding to mannose receptors (CD206) expressed on reticuloendothelial cells residing in lymph nodes [7]. The CD206 receptor, mannose receptor C type 1 or MRC1, recognizes and binds macromolecules with carbohydrate side-chains terminating in a mannose glycoside [8]. Theoretically specific binding to receptors resident in the lymph node would allow a small molecule with rapid clearance from the primary injection site and rapid transit to the regional node to bind with high affinity and accumulate in the first node it encountered – the ‘sentinel’ node. When combined with an appropriate radiolabel for imaging, this receptor-targeted agent would have potential advantages over nonspecific colloids.
■Chemistry
Vera et al. first described the synthesis of 99mTcdiethylenetriaminepentaacetic acid (DTPA)- mannosyl-dextran in 2001 [7]. The agent was subsequently referred to as Lymphoseek, and later given the generic name 99mTc-tilmanocept. Vera and colleagues’ initial report described high labeling yields (in excess of 98%) and stability, and very high receptor binding affinity. The equilibrium dissociation binding constant KD in a rat liver assay was 0.12 ± 0.07 nM. The macromolecule had an average molecular weight of 28,200–35,800 g/mol [7,9], with the current formulation as tested in Phase III clinical trials being 18,000 g/mol. The molecular diameter was 7.1 nm. Dextran is very hydrophilic, which combined with the relatively low molecular weight and diameter, promotes rapid clearance of 99mTc-tilmanocept from the injection site via both lymphatic and blood capillaries [7].
■Preclinical studies
Biodistribution studies in rabbits indicated that 99mTc-tilmanocept cleared the foot pad with a biological half-life of 2.21 ± 0.27 h [10], and comparison studies with filtered 99mTc-sulfur colloid revealed faster injection site clearance and lower accumulation in distal lymph nodes, but similar accumulation in the proximal nodes at 1 and 3 h after injection [7]. Biodistribution was also tested in pigs after endoscopic injection into the stomach, colon and prostate gland [11–14]. The experiments confirmed relatively rapid transit to initial draining lymph nodes, good correlation with vital blue dye staining and low uptake in distal lymph nodes.
Preclinical toxicology studies were conducted in rats and rabbits after footpad administration, and in rabbits following intramuscular or intravenous administration, using between 50- and 1000-times the scaled human dose. Other than mild hepatocyte hypertrophy in rabbits, no abnormalities in toxicology or pathology were seen. Intravenous and intramuscular administration had no effect on survival, ECGs or blood pressure [10].
Clinical studies – Phase I: biodistribution & safety
The biodistribution and safety of 99mTc-tilmanocept at various doses were tested in 18 female breast cancer patients, and compared with six additional patients who received filtered 99mTcsulfur colloid [15]. Dose-dependent sentinel node uptake was observed and injection site clearance of 99mTc-tilmanocept was similar across doses. 99mTc-tilmanocept exhibited a significantly faster injection site clearance: the mean 99mTc-tilmanocept clearance half-time was 2.72 ± 1.57 h compared with 49.5 ± 38.5 h for filtered 99mTc-sulfur colloid (p < 0.0025) [9]. The mean sentinel node uptake, however, was not statistically significantly different for 99mTc-tilmanocept versus sulfur colloid; in fact, the values were slightly higher for filtered 99mTc-sulfur colloid [9,16]. The mean number of sentinel nodes detected was 1.3 and 1.7 for 99mTc-tilmanocept and filtered 99mTc-sulfur colloid, respectively [9].
Wallace et al. also conducted a Phase I trial of 99mTc-tilmanocept in patients with clinically localized melanoma [17]. In this trial, 24 patients received intradermal injections of 99mTc-tilmanocept (six patients each received 1.0, 5.0 or 10.0 nmol) or filtered 99mTc-sulfur colloid. Again, 99mTc-tilmanocept exhibited a significantly faster injection site clearance: the mean clearance half-time for all three 99mTc-tilmanocept groups was 2.17 ± 0.96 h compared with 14.7 ± 6.3 h for filtered 99mTc-sulfur colloid (p < 0.001). As in the breast cancer experience, mean sentinel node uptake was not statistically significantly different for 99mTc-tilmanocept versus 99mTc-sulfur colloid and the mean number of sentinel nodes detected was slightly, but not statistically significantly, lower for 99mTc-tilmanocept.
Another publication described results comparing the injection site clearance and sentinel lymph node accumulation after a single intradermal injection of 99mTc-tilmanocept or unfiltered 99mTc-sulfur colloid using a 2-day protocol for breast cancer lymphoscintigraphy and lymphatic mapping [18]. A total of 11 patients with breast cancer received either an intradermal administration of 1.0 nmol of 99mTc-tilmanocept or unfiltered 99mTc-sulfur colloid and underwent surgery the next day. 99mTc-tilmanocept exhibited significantly faster injection site clearance than unfiltered 99mTc-sulfur colloid and demonstrated persistent accumulation in the sentinel node for at least 24 h. The mean sentinel lymph node uptake of 99mTc-tilmanocept was lower than unfiltered 99mTc-sulfur colloid (1.5 ± 1.7 vs 3.5 ± 3.1%), but again this difference was not statistically significant (p = 0.213). No serious adverse events related to 99mTc-tilmanocept were identified in any of the Phase I trials. Faster clearance from the injection site could potentially enhance the detection of sentinel nodes by decreasing ‘shine through’ from the primary site, but this remains an unproven theoretical consideration.
Clinical studies: Phase II & III: clinical efficacy
Clinical testing initially took place in a series of small Phase I trials, some involving a randomized comparison with filtered 99mTc-sulfur colloid (see above). This was followed by a multiinstitutional open-label Phase II trial involving patients with melanoma or breast cancer undergoing clinically indicated sentinel node biopsy [19]. More recently, two nonrandomized Phase III trials, nearly identical in design, were completed in patients with either breast cancer or melanoma, and a third nonrandomized Phase III trial is currently underway in patients with squamous cell carcinoma of the head and neck. None of the completed Phase II and III trials involved a direct or indirect comparison with any other radiolabeled lymphatic-mapping agent, but they did provide comparative data to isosulfan blue dye.
Breast cancer & melanoma
In a prospective, nonrandomized Phase II trial, Leong et al. reported on 78 patients (47 with melanoma and 31 with breast cancer) who received 99mTc-tilmanocept as part of clinically indicated sentinel lymph node biopsy procedures [19]. In 55 patients, preoperative lymphoscintigraphy was performed, and a ‘hot spot’ indicative of a sentinel node or nodes was identified in 94.5% of these patients. Intraoperatively, 99mTc-tilmanocept identified at least one sentinel node in 75 out of 78 patients (96.2%), and 175 out of the 182 nodes removed at surgery (95.1%) were radioactive. Out of 26 tumor-positive nodes removed, 25 were identified by 99mTc-tilmanocept; one breast cancer patient had a tumor-positive node that was not radioactive. Five serious adverse events occurred in this trial, but all were considered to be related to the surgical procedure and none were attributed to the administration of 99mTc-tilmanocept. Only three patients (3.8%) experienced adverse events that were considered possibly related to the 99mTc-tilmanocept; no patient had an adverse event considered definitely or possibly related, and there were no deaths on the study.
Two very similar nonrandomized Phase III trials, NEO3-05 and NEO3-09, were completed in patients with either breast cancer or melanoma, and have been presented in abstract form at the American Society of Clinical Oncology [20] and the Society for Nuclear Medicine [21]. These trials were designed in consultation with the US FDA with the intent of serving as registration trials for 99mTc-tilmanocept. At the time of the studies’ design and conduct, the only FDA-approved agent for lymphatic mapping was isosulfan blue dye (or Patent Blue V®, approved in Europe), therefore, this agent was selected as the withinpatient comparator and concordance with the blue dye was the primary end point. Subsequent to the completion of the Phase III trials, the FDA approved 99mTc-sulfur colloid for the localization of lymph nodes draining a primary breast cancer or melanoma, based on retrospective data demonstrating a high level of concordance with vital blue dye (see the ‘Regulatory affairs’ section below).
In both Phase III trials, involving a total of 332 patients with primary melanoma or breast cancer, 99mTc-tilmanocept (50 μg at 0.5–1.0 mCi 99mTc) provided superior results compared with vital blue dye. Each patient was to undergo a preoperative injection of 99mTc-tilmanocept with lymphoscintigraphy, then intraoperative injection of vital blue dye. As in most tilmanocept studies, total volume was not fixed, but instead adjusted to provide the required nanomolar concentration. Intraoperative lymphatic mapping was performed with a handheld g-detector (Neoprobe, Devicor Medical Products Inc., OH, USA), using strict criteria (the ‘3-sigma rule’, as described in [22]) to define radioactive nodes and visual evaluation for the presence of blue dye within nodes. All radioactive, blue or palpably abnormal nodes were excised and examined histologically. The ‘intentto- treat’ group was defined as those patients with at least one blue node who had also received an injection of 99mTc-tilmanocept, as these were the patients who were evaluable for the primary end point of concordance of 99mTc-tilmanocept with blue dye. A reverse-concordance group was defined to consist of patients with at least one radioactive node who also received an injection of blue dye. The prespecified null hypothesis was that concordance was ≤0.90, while the alternative hypothesis was concordance >0.90, using a two-sided test for significance at the a = 0.05 level.
In both trials, 99mTc-tilmanocept was highly concordant with blue dye: over 95% of blue nodes were radioactive using the 3-s definition, and, therefore, the null hypothesis of concordance being 90% or less was rejected statistically, meeting the prespecified end point for concordance. By contrast, reverse concordance was poor: many radioactive nodes were not visibly blue. More radioactive nodes were identified and removed than blue nodes, and a few tumorcontaining nodes were radioactive but not blue. No tumor-containing nodes were blue but not radioactive, although two palpable nodes containing breast cancer in one patient were neither radioactive nor blue. Detailed results for each trial as prospectively conducted have not been published, but recent publications have provided aggregated results for the two trials subdivided by tumor type.
A combined analysis of the melanoma patients enrolled onto these two Phase III trials has been reported [22]. A total of 154 melanoma patients from 15 centers were injected with both agents and evaluated intraoperatively. A total of 232 out of 235 blue nodes were detected by 99mTc-tilmanocept intraoperatively for 98.7% concordance with blue dye (p < 0.001 that the true concordance rate exceeds 90%). 99mTc-tilmanocept detected 364 nodes as ‘hot’ for 63.7% reverse concordance (232 out of 364 hot nodes were also blue). 99mTc-tilmanocept detected at least one node in more patients (n = 150) than blue dye (n = 138; p = 0.002). In 135 out of 138 patients with at least one blue node, all blue nodes were radioactive. Melanoma was identified in the sentinel nodes of 22.1% of patients; all 45 melanoma-positive sentinel nodes were detected by 99mTc-tilmanocept, whereas blue dye detected only 36 (80%) out of 45 nodes (p = 0.004). No melanoma-positive sentinel nodes were detected exclusively by blue dye. Four out of 34 node-positive patients were identified by 99mTc-tilmanocept only, therefore, four (2.6%) out of 154 patients were correctly staged by 99mTc-tilmanocept only. No serious adverse events were attributed to 99mTc-tilmanocept [22].
Another recent publication looked at the efficacy of 99mTc-tilmanocept in sentinel lymph node identification in breast cancer patients [23]. Concordance data from the two Phase III clinical trials of 99mTc-tilmanocept plus vital blue dye was compared with a meta-analysis of a review of the literature pertaining to ‘standard of care’ 99mTc-labeled nanocolloid human serum albumin (Nanocoll®, GE Healthcare Ltd, Buckinghamshire, UK). Five studies involving 6134 breast cancer patients were reviewed to calculate the aggregate sentinel node identification rate of 95.9% for 99mTc-labeled nanocolloid human serum albumin (estimated 95% CI: 94.3–97.5%). Three studies involving 1380 patients were included to calculate the number of sentinel nodes per procedure identified with 99mTc-labeled nanocolloid human serum albumin of 1.67 nodes (95% CI: 1.51–51.82). The lower bound of the CI was used for comparison with 99mTc-tilmanocept. The Phase III 99mTc-tilmanocept data included 148 breast cancer patients, and pooled analysis revealed a 98.65% sentinel node identification rate (95% CI: 95.0–99.8%) with pooled 2.16 lymph nodes per procedure (95% CI: 1.96– 92.36). Using a comparison of the lower bound values of the 95% CIs, the authors concluded that 99mTc-tilmanocept was statistically superior to 99mTc-labeled nanocolloid human serum albumin for both the rate of sentinel node identification and the number of nodes identified per procedure (p < 0.001 and p = 0.008, respectively) [23]. The authors note several limitations inherent in this type of pooled analysis and retrospective review, not least of which is the variability in defining a sentinel lymph node as radioactive during standard of care surgical procedures compared with the prescribed use of standardized definitions in a prospective trial.
Head & neck squamous cell carcinoma
The two Phase III trials involving breast cancer and melanoma patients met their prespecified regulatory end points of concordance, but the trials were not designed to estimate how often neither blue dye nor 99mTc-tilmanocept identified tumor-containing nodes (i.e., how often the sentinel node procedure was falsely negative). Since complete lymphadenectomy is no longer performed for clinically node-negative breast cancer or melanoma patients unless a sentinel node is found to contain malignancy, directly estimating the ‘false negative’ rate of 99mTc-tilmanocept is not feasible in these patients. A nonrandomized Phase III trial was designed to address this issue in patients with squamous cell carcinomas of the head and neck, either of cutaneous or upper aerodigestive tract origin, who were undergoing clinically indicated complete cervical lymphadenectomy for clinically nodenegative cancers. This trial is open and accruing patients (trial identifier NCT00911326), but as yet no results are available [101].
Other solid tumors
At the time of writing this article, no prospective clinical trials of 99mTc-tilmanocept have been conducted or are known to be planned in patients with any other tumor types.
Safety & tolerability
Overall, the reported data – particularly from Phase II and III evaluations of 99mTc-tilmanocept alone or in combination with vital blue dye – suggest this agent is safe and very well tolerated. No agent-specific serious adverse events have been identified, and most of the reported adverse events in the Phase II and III trials appear to have been associated with the sentinel node biopsy procedure rather than 99mTc-tilmanocept. Whether tilmanocept is more tolerable than currently used colloids has not been systematically evaluated, although it has been suggested that it could be associated with less injection site discomfort than filtered 99mTcsulfur colloid [19]. Demonstrating improved tolerability, however, would require prospective comparisons (ideally randomized) involving additional numbers of patients.
Regulatory affairs
Until very recently, none of the colloids commonly used for intraoperative sentinel node identification around the world were specifically approved for that purpose. Isosulfan blue dye is approved by the FDA for lymphatic identification and hence has featured prominently in the design of Phase III trials intended to support registration of 99mTc-tilmanocept specifically for this purpose. In July 2011, the FDA granted approval to Pharmalucence Inc. (MA, USA) to add the location of lymph nodes in breast cancer patients to the label indications for its 99mTc-sulfur colloid product [102]. This approval was based not on prospective trial data, but rather on a systematic literature review involving 15 ‘prospectively designed studies’ reporting results from 9213 breast cancer sentinel node procedures. Overall, 99mTc-sulfur colloid was present in at least one lymph node in 94.1% of procedures, while blue dye was present in at least one lymph node in only 85.1%. Furthermore, 99mTc-sulfur colloid in conjunction with blue dye was also superior to blue dye alone in this analysis [102]. Subsequently, in August 2012, the FDA added localization of lymph nodes in melanoma to the label indications for the Pharmalucence Inc. 99mTc-sulfur colloid for injection, based on similar literature review data [103]. On 13 March 2013, the FDA approved 99mTc-tilmanocept (Lymphoseek injection) as a radioactive diagnostic agent indicated for lymphatic mapping with a handheld g counter to assist in the localization of lymph nodes draining a primary tumor site in patients with breast cancer or melanoma [104].
The FDA’s decision to approve 99mTc-sulfur colloid has potential implications for the future of 99mTc-tilmanocept. By accepting a nonrandomized comparison with vital blue dye as the basis for approval, the case for approval of 99mTc-tilmanocept based on rigorous prospective clinical trial data was markedly strengthened. On the other hand, the fact that 99mTc-sulfur colloid is now approved for breast cancer and melanoma lymphatic mapping may increase the pressure from practitioners or payors (and even some regulatory agencies worldwide) to directly demonstrate the advantages of 99mTc-tilmanocept over 99mTc-sulfur colloid in prospective, randomized trials. Of course, this would be influenced by the cost, convenience and potential for reimbursement when 99mTc-tilmanocept is brought to market.
Conclusion & future perspective
99mTc-tilmanocept is an interesting agent designed specifically for the pre- and intra-operative identification of sentinel lymph nodes. Sentinel node biopsy is widely used globally in the management of breast cancer and melanoma, and may have a role in a variety of other solid tumors. In most of the world, no radiopharmaceutical is approved specifically for use in this procedure, and no new imaging agents have been introduced into clinical practice for more than a decade. Therefore, the availability of a new agent with advantages over current alternatives is of great potential interest. The clinical trial data available to date support the conclusion that 99mTc-tilmanocept is an effective and safe agent for identifying sentinel lymph nodes in melanoma and breast cancer; however, it remains unclear how much of an improvement, if any, it will represent over traditional agents.
Acknowledgements
A portion of the abstract has been reproduced with permission from John Wiley & Sons, Inc. [24].
Financial & competing interests disclosure
The authors were participating investigators in two Phase III trials of tilmanocept in melanoma, and Moffitt Cancer Center (FL, USA) received funding to support the costs associated with those research trials. V Sondak has been a paid consultant to Navidea. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
- Morton DL, Wen DR, Wong JH et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch. Surg. 127(4), 392–399 (1992).
- Morton DL, Thompson JF, Cochran AJ et al. Sentinel-node biopsy or nodal observation in melanoma. N. Engl. J. Med. 355(13), 1307–1318 (2006).
- Kamath D, Rapaport D, DeConti R et al. Redefining cutaneous lymphatic flow: the necessity of pre-operative lymphoscintigraphy in the management of malignant melanoma. J. Fla. Med. Assoc. 84(3), 182–187 (1997).
- Reynolds HM, Dunbar PR, Uren RF, Blackett SA, Thompson JF, Smith NP. Three-dimensional visualization of lymphatic drainage patters in patients with cutaneous melanoma. Lancet Oncol. 8(9), 806–812 (2007).
- Zager JS, Puleo CA, Sondak VK. What is the significance of the in transit or interval sentinel node in melanoma? Ann. Surg. Oncol. 18(12), 3232–3234 (2011).
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J. Clin. 61, 69–90 (2011).
- Vera DR, Wallace AM, Hoh CK, Mattrey RF. A synthetic macromolecule for sentinel node detection: 99mTc-DTPA-mannosyl-dextran. J. Nucl. Med. 42(6), 951–959 (2001).
- Figdor CG, van Kooyk Y, Adema GJ. C-type lectin receptors on dendritic cells and Langerhans cells. Nat. Rev. Immunol. 2(2), 77–84 (2002).
- Wallace AM, Hoh CK, Vera DR, Darrah DD, Schulteis G. Lymphoseek: a molecular radiopharmaceutical for sentinel node detection. Ann. Surg. Oncol. 10(5), 531–538 (2003).
- Hoh CK, Wallace AM, Vera DR. Preclinical studies of [99mTc]DTPA-mannosyl-dextran. Nucl. Med. Biol. 30(5), 457–464 (2003).
- Méndez J, Wallace AM, Hoh CK, Vera DR. Detection of gastric and colonic sentinel nodes through endoscopic administration of 99mTc-DTPA-mannosyl-dextran in pigs. J. Nucl. Med. 44(10), 1677–1681 (2003).
- Ellner SJ, Méndez J, Vera DR, Hoh CK, Ashburn WL, Wallace AM. Sentinel lymph node mapping of the colon and stomach using lymphoseek in a pig model. Ann. Surg. Oncol. 11(7), 674–681 (2004).
- Salem CE, Hoh CK, Wallace AM, Vera DR. A preclinical study of prostate sentinel lymph node mapping with [99mTc] diethylenetetramine pentaacetic acidmannosyl- dextran. J. Urol. 175(2), 744–748 (2006).
- Wallace AM, Ellner SJ, Méndez J et al. Minimally invasive sentinel lymph node mapping of the pig colon with Lymphoseek. Surgery 139(2), 217–223 (2006).
- Ellner SJ, Hoh CK, Vera DR, Darrah DD, Schulteis G, Wallace AM. Dose-dependent biodistribution of [99mTc]DTPA-mannosyldextran for breast cancer sentinel lymph node mapping. Nucl. Med. Biol. 30(8), 805–810 (2003).
- Wallace AM, Hoh CK, Darrah DD, Schulteis G, Vera DR. Sentinel lymph node mapping of breast cancer via intradermal administration of Lymphoseek. Nucl. Med. Biol. 34(7), 849–853 (2007).
- Wallace AM, Hoh CK, Ellner SJ, Darrah DD, Schulteis G, Vera DR. Lymphoseek: a molecular imaging agent for melanoma sentinel lymph node mapping. Ann. Surg. Oncol. 14(2), 913–921 (2007).
- Wallace AM, Hoh CK, Limmer KK, Darrah DD, Schulteis G, Vera DR. Sentinel lymph node accumulation of Lymphoseek and Tc-99m-sulfur colloid using a ‘2-day’ protocol. Nucl. Med. Biol. 36(6), 687–692 (2009).
- Leong SP, Kim J, Ross M et al. A Phase 2 study of 99mTc-tilmanocept in the detection of sentinel lymph nodes in melanoma and breast cancer. Ann. Surg. Oncol. 18(4), 961–969 (2011).
- Cope FO, Sondak VK, Wallace AM. A Phase III study of receptor-targeted 99mTc-tilmanocept versus blue dye in the evaluation of SLNs in breast cancer and melanoma. J. Clin. Oncol. 29(18S Suppl. II), 783s (2011).
- Sondak VK, Wallace A. A prospective open label Phase 3 trial of receptor-targeted 99mTc-tilmanocept for sentinel node evaluation in breast cancer and melanoma. J. Nuc. Med. 52(Suppl. 1), 599 (2011).
- Sondak VK, King DW, Zager JS et al. Combined analysis of Phase III trials evaluating [99mTc]tilmanocept and vital blue dye for identification of sentinel lymph nodes in clinically node-negative cutaneous melanoma. Ann. Surg. Oncol. 20(2), 680–688 (2013).
- Tokin CA, Cope FO, Metz WL et al. The efficacy of tilmanocept in sentinel lymph mode [sic] mapping and identification in breast cancer patients: a comparative review and meta-analysis of the 99mTc-lableled nanocolloid human serum albumin standard of care. Clin. Exp. Metastasis 29, 681–686 (2012).
- Sondak VK. New lymphatic mapping agents. Pigment Cell Res. 24(15), 1010 (2011) (Abstract).


