Review Article - Imaging in Medicine (2011) Volume 3, Issue 5
The use of 4D imaging in the behavioral assessment of high-risk fetuses
Asim Kurjak†1,2, Maja Predojević3, Milan Stanojević4, Amira Talić5, Ulrich Honemeyer6 and Aida Salihagić Kadić3,71Department of Obstetrics& Gynecology, Clinical Hospital Sveti Duh, Medical School, University of Zagreb, Zagreb, Croatia
2Department of Obstetrics& Gynecology, Fetomaternal Unit, Hamad Medical Corporation, Doha, Qatar
3Department of Physiology, Medical School, University of Zagreb, Zagreb, Croatia
4Division of Neonatology, Department of Obstetrics & Gynecology, Clinical Hospital ‘‘Sveti Duh’’, Zagreb, Croatia
5Department of Obstetrics & Gynecology, University of Medical Sciences & Technology, Academy Charity Hospital, Khartoum, Sudan
6University of Medical Sciences & Technology, Khartoum, Sudan& Welcare Hospital, Dubai, UAE
7Croatian Institute for Brain Research, Medical School, University of Zagreb, Zagreb, Croatia
- *Corresponding Author:
- Asim Kurjak
Department of Obstetrics& Gynecology Clinical Hospital Sveti Duh
Medical School University of Zagreb, Zagreb, Croatia
E-mail: asim.kurjak@zg.htnet.hr
Abstract
Fetal behavioral patterns have been considered as indicators of fetal brain development. Numerous studies employing conventional 2D ultrasound have shown that normally developing fetuses and fetuses at risk exhibit different patterns of behavior. With the appearance and development of 4D ultrasound, fetal behavioral movements, and the full range of facial expressions can be observed. After standardization of valid reference ranges of movements appropriate for the gestational age, the Zagreb group published a new scoring system for fetal neurobehavior based on prenatal assessment by 4D sonography, the Kurjak Antenatal Neurological Test. The aims and objectives of this article were to describe the latest 4D sonographic studies on fetal behavior and to present results of behavioral assessment by KANET in high-risk pregnancies.
Keywords
4D ultrasound; development of CNS; fetal behavior; general movements; prenatal neurological test
Fetal behavior can be described as any fetal action or reaction observed by the mother or more objective method, such as ultrasonography [1]. Analysis of the fetal dynamics in comparison with morphological studies led to the conclusion that fetal behavior reflects the activity of the fetal CNS [2]. Therefore, it was assumed that the evaluation of fetal behavior in different periods of gestation might give the possibility to differentiate normal from abnormal brain development, and enable early diagnosis of various structural or functional abnormalities [3]. 2D sonography improved our understanding of fetal behavior, the real breakthrough in this area was achieved by 4D ultrasound, as will be presented later in this article.
Basic principles of 4D sonography in the assessment of fetal behavior
4D ultrasound displays a continuously updated and newly acquired volume in any rendering modality, creating the impression of a moving structure. 4D ultrasound examination starts in the conventional real-time 2D mode. At first, a real-time 2D imaging appears on the monitor, alongside the continuously updated near realtime image. Once the displayed sequences are deemed satisfactory, the operator can activate a full-screen display of the moving surface rendering [4].
As 4D imaging is almost a real time, there is always some delay as a result of time required to reconstruct 3D images from 2D scans. Prior to volume acquisition it is important to achieve the best 2D image quality, as all the 2D image artifacts will also be present on 3D and 4D image reconstruction [5]. An important limiting factor for 4D sonography is the amount of amniotic fluid.
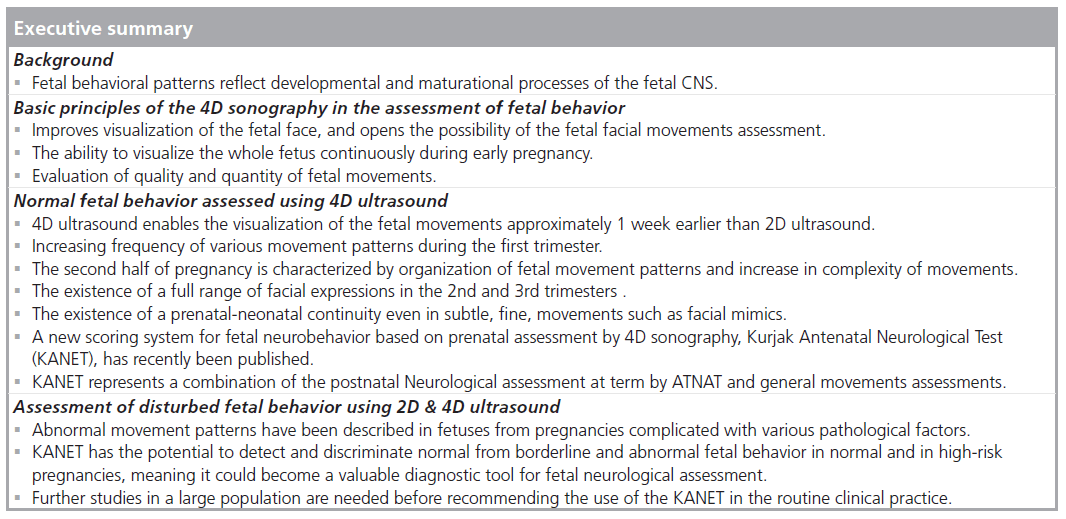
Ultrasound in general provides dynamic imaging of the human body. Modern ultrasound technology, such as 4D sonography, enables study of the fetal activity in the surface-rendering mode, improves visualization of the fetal face, and opens the possibility of assessment of the fetal facial movements [6]. With 4D ultrasound, it is now feasible to study a full range of facial expressions including smiling, crying, scowling and eyelid movements [7,8]. Simultaneous imaging of complex facial movements was not possible using real-time 2D ultrasound. 4D ultrasound integrates the advantage of the spatial imaging of the fetal face with the addition of time. This new technology therefore allows detailed imaging of the each fetal facial movement in time. The observation of facial expression may be of scientific and diagnostic value [9].
The additional advantage of 4D ultrasound in comparison with 2D ultrasound is the ability to visualize the whole fetus continuously during early pregnancy. In addition, the introduction of high-frequency transvaginal transducers has resulted in remarkable progress in ultrasonographic visualization of embryos and early fetuses. For the first-time parallel analysis of structural and functional parameters in the first 12 weeks of gestation have become possible. In the early second trimester 4D ultrasound provides simultaneous visualization of all four extremities and enables confident recognition of isolated arm movements and their direction. The key benefit of 4D ultrasound lies in providing real-time 3D images of embryonic or fetal movements. Owing to the limitations of 2D ultrasound only five types of isolated hand movements could be described. They include: hand to head, hand to trunk, hand to foot, hand to fluid and hand to the uterine wall. If one performs 4D ultrasound hand to head movement can be differentiated into seven subgroups: hand-to-head, hand-to-mouth, hand-near-mouth, hand-to-face, hand-near-face, hand-to-eye and hand-to-ear [10]. Furthermore, using 4D ultrasound in obstetrics, it is possible for the first time to monitor quality and quantity of fetal movements on 3D real-time reconstructed images.
It is our belief that 4D ultrasound should have its place in everyday obstetric practice, combining patient acceptance and sensitivity of diagnosis. One of the possible applications of 4D sonography is analysis of fetal behavior in order to reach assessment of functional development of the CNS as a measure of neurological maturation.
Normal fetal behavior assessed by 4D ultrasound
Ultrasonic studies have revealed that fetal activity occurs far earlier than it can be registered by the mother, during the late embryonic period. Early embryonic development is characterized by the immobility of an embryo, between 7 and 15 weeks of gestation, most types of movement pattern will emerge [11]. Based on the first analysis of fetal movements by 2D ultrasonography, de Vries classified movements into different patterns as follows [12,13]: sideways bending, startle, general movements (GMs), hiccups, breathing-like movements, isolated arm or leg movement, twitches, clonic movements, isolated retroflexion of the head, isolated rotation of the head, isolated anteflexion of the head, jaw movements, sucking and swallowing, hand– head contact, stretching, yawning, rotation of the fetus. One of the important prerequisites for the motility is the development of the CNS structures (for better understanding of these processes see [14]).
First spontaneous fetal movements can be observed with conventional 2D ultrasound at approximately the 8th gestational week. However, 4D ultrasound allows the visualization of fetal motility at 7 weeks of gestation [11,15–17]. Obviously, this new technology enables the visualization of the moving phenomenon about 1 week earlier than 2D ultrasound.
General movements are the first complex fetal movement patterns [13]. They can be recognized from 8–9 weeks of pregnancy and continue to be present until 16–20 weeks after birth [18]. These movements involve the whole body [19]. Movements of the limbs, trunk and head are of variable speed, but smooth in appearance. They wax and wane in intensity, force and speed and they have a gradual beginning and ending [19]. 4D ultrasound significantly enhanced assessment of quality of GMs. During early pregnancy this technology allows the simultaneous visualization of fetal head trunk and limbs. The majority of sequences of extension and flexion of the legs and arms is complex, and may be better assessed. Furthermore, 4D sonography seems to be the method of choice for detecting subtle changes, such as superimposed rotations and changes in direction of the movements. These additional components make the movements more fluent and elegant and create the impression of complexity and variability.
The first appearance of limb movements is between 8th and 12th weeks of gestation [11,13,15–17,20,21]. With 4D ultrasound, limb movements were found after 10 weeks of gestation [20]. The organization of this movement pattern occurs with the increase in gestation [22]. The movements in the elbow joint appear at 10 weeks, changes in finger position at the 11th week, and easily recognizable clenching and unclenching of the fist at 12–13 weeks. Finally, at 13–14 weeks, isolated finger movements can be observed, as well as increase in the activity and strength of the hand/finger movements [23]. Using 4D sonography, Kurjak and collaborators have found that from 13 gestational weeks onwards, a ‘goal orientation’ of hand movements appears and a target point can be recognized for each hand movement [10]. According to the spatial orientation, they classified the hand movements into several subtypes: hand-to-head, hand-to-mouth, hand-near-mouth, hand-to-face, hand-near-face, hand-to-eye and hand-to-ear.
Besides the general body movements and isolated limb movements, hiccups, sucking, and swallowing movements can be seen from the 9th week of gestation. Further, retroflexion, anteflexion, rotation of the head, breathing-like movements, jaw opening and yawning can be observed during the 10th week of gestation. From 10 weeks onwards, the number and frequency of fetal movements increase and the repertoire of movements begins to expand as a result of the CNS structures maturation (for references see [14]).
Our longitudinal study, performed by the 4D ultrasound in 100 fetuses from all trimesters of normal pregnancies, has shown increasing frequency of various movement patterns, such as GMs, isolated arm and leg movements, stretching, as well as head movements, during the first trimester. Only the startle movement pattern seemed to occur stagnantly in this period of gestation [24]. Using 4D sonography, GMs were found to be the most frequent movement pattern between 9 and 14 weeks of gestation [17].
In the recent 4D sonographic study, Hata et al. showed that the most common movements at 10–11 weeks of gestation were isolated arm movement, and at 12–13 weeks jumping movement [25]. Authors provided possible explanation of the difference between this study and previous investigations in terms of behavior patterns assessed. As stated by Hata et al., “It is important to bear in mind that more shortduration isolated movements might constitute more pronounced fetal movements in early gestation, whereas whole-body movements that are characteristic of the mature fetus may constitute greater movements in late gestation. However, whole-body movements are actually a composite of isolated body movements” [26], and it may be important to standardize the definition of behavior patterns for future studies. According to authors, another possible explanation is the difference in the frame rates of the machines used in the studies. The frame rate was 0.5/s in all previous investigations, whereas in this study it was 2.6–4.0/s. A final potential explanation by the authors was the small number of subjects in studies, and concludes that further research involving a larger sample is required to evaluate the exact frequencies of fetal movement in the first trimester of pregnancy [25].
From 14 to 19 weeks of gestation, the fetuses are highly active and the longest period between movements last only 5–6 min (for references see [14]). According to Kuno et al., the most active fetal behavior pattern between 14 and 18 weeks of gestation was an arm movement, whereas the least was a mouth movement. Furthermore, the active phase (time with fetal movements) was 59.4%, and the resting phase was 40.6% during 60 min of recording [27]. In the 15th week, 16 different types of movement can be observed (for references see [14]). Furthermore, at 16–18 weeks of gestation the earliest eye movements appear as sporadic movements with a limited frequency [28,29]. From 20 to 22 weeks of gestation fetal movements, breathing-like activity, and heart rate begin to follow daily cycles called circadian rhythm [30]. The second half of pregnancy is characterized by organization of fetal movement patterns and increase in complexity of movements. The periods of fetal quiescence begin to increase, and the rest-activity cycles become recognizable. Hardly any new movement patterns emerge in this period. The number of general body movements, which tends to increase from the 9th week onwards, gradually declines during the last 10 weeks of the pregnancy [31–33]. It is very important to point out that GMs are characterized by large variation and complexity in the third trimester [34]. Simultaneously with the decrease in the number of GMs, an increase in facial movements, including opening/ closing of the jaw, swallowing and chewing, was observed using 2D sonography between 28 and 38 weeks of gestation. These movements appeared mostly in the periods of absence of generalized movements, and such pattern was considered to be a reflection of the normal neurologic development of the fetus [31].
Using 3D/4D sonography, our results confirmed the value of this technology in the investigation of structural and functional development of the fetal face [9]. The application of 4D sonography in the examination of fetal facial movements has revealed the existence of a full range of facial expressions, including smiling (Figure 1), and crying [7,24], similar to emotional expressions in adults, in the 2nd and 3rd trimester. Other facial movements, such as yawning (Figure 2), sucking, swallowing and jaw opening can also be observed in this period by 4D ultrasound. According to Yan et al., mouthing was the most frequent facial movement during early third trimester, whereas the least frequent were scowling and sucking [35]. Our longitudinal analysis of the frequencies of different facial movements in the 2nd and 3rd trimester revealed some interesting results. Contrary to the declining trend of head movement and hand movement patterns from the beginning of the second trimester to the end of the third trimester, a constant increase in the frequencies of almost all facial motor patterns was observed during the 2nd trimester. Various types of facial expression patterns displayed a peak frequency at the end of 2nd trimester, except eye blinking pattern (Figure 3). During the remainder of pregnancy, decreasing or stagnant incidence of facial movement patterns was noted [24].

Figure 1. Image of the fetus recorded by 3D/4D sonography showing smiling movement. Reproduced with permission from [74].

Figure 2. A sequence of images of the fetus recorded by 3D/4D sonography showing yawning. Reproduced with permission from [74].

Figure 3.A sequence of images of the fetus recorded by 3D/4D sonography showing eye blinking movement. Reproduced with permission from [74].
At 36–38 weeks of gestation, eye movements become integrated with other parameters of fetal activity, such as heart rate and fetal movements, into organized, coherent behavioral states [36,37].
A further challenge was to determine what proportion of fetal movements resembles those seen in preterm and term infants. Authors found no statistically significant differences in either quality or quantity of fetal hand-toface movements or fetal facial movements. There were no movements observed in fetal life that were not present in neonates. This study confirmed the existence of a prenatal–neonatal continuity even in subtle, fine, movements such as facial mimics [22].
During the last decade, 4D sonography has stimulated studies on fetal behavior with more convincing imaging and data than those obtained by conventional ultrasonic and nonultrasonic methods [38,39]. The findings indicate that a good understanding of the relationship between fetal behavior and developmental processes in different periods of gestation might provide an important distinction between normal and abnormal brain development, and enable early diagnosis of structural or functional abnormalities [3]. Contrary to this obvious fact, the idea of diagnosis in utero of some functional neurological disorders was very intriguing. The latest knowledge in the intriguing area of normal and pathological development of the fetal CNS is described in a recently published book [40].
Recently, a new scoring system for fetal neurobehavior based on prenatal assessment by 3D/4D sonography has been suggested [41]. This new test was named after the first author Kurjak Antenatal Neurological Test (KANET). KANET was developed after discussions and consensus between members of an international collaborative project [24,42], and represents a combination of the postnatal The Amiel-Tison Neurological Assessment at Term (ATNAT) and GMs assessments [19,43–47].
ATNAT takes into account neurological maturation, exploring a so-called lower subcortical system whose essential role is to maintain posture against gravity and flexor tone in the limbs [44,48]. The upper system controls the lower system, with relaxation of the limbs and control of the antigravity forces, finally allowing erect posture, walking and fine motor skills [49]. ATNAT consists of: head circumference measurement, assessment of cranial sutures, visual pursuit, social interaction, sucking reflex, raise-to-sit and reverse, passive tone in the axis, passive tone in the limbs, fingers and thumbs outside the fist, and autonomic control during assessment [48]. The ATNAT is increasing accuracy in assessing CNS function in the neonate by using a simple scoring system, focusing on the most meaningful items, promoting a clinical synthesis at term, for term and preterm infants [48]. Similarity between neonatal optimality test of Amiel-Tison and the new scoring system can be observed in assessments of head growth parameters including sutures’ status, primary ref lexes, (restricted to sucking behavior), finger movements and abduction of thumbs [50]. Some criteria observed in the fetus are only prerequisites for ex utero functional achievements: opening of the eyes for visual pursuit, and facial expressions for social interaction. Their identification by 4D imaging, in addition to efficient and rhythmic sucking supports the absence of CNS depression [50]. However, analytical criteria of typical passive and active tone in the neonate cannot be elicited in the fetus: head anteflexion versus retroflexion, ventral versus dorsal incurvations in the axis, both being of the utmost importance postnatally to confirm CNS optimality. Still, optimality in the fetus should be reflected in typical GMs [50].
The observation of pre- and post-natal spontaneous motor behavior drove Prechtl to describe GMs as a “series of gross movements of variable speed and amplitude, which involve all parts of the body but lack a distinctive sequencing of the participating body parts”. According to this author any brain damage will interfere with the endogenous motor activity [3,43,51–54]. Indeed, alterations of spontaneous GMs can be observed in preterm and term newborns with cerebral impairment (for references see [14]). Their movements seem to lose the characteristic fluency and complexity, and become cramped and unsynchronized. In addition, assessment of GMs at so-called fidgety GM age has been found to have the highest predictive value for development of cerebral palsy (CP), if abnormal [3,55]. Lack of fluency and existence of considerable variation and complexity are the main characteristics of mildly abnormal GMs [56]. When complexity, variation and fluency are absent, we are dealing with definitely abnormal GMs [56]. Therefore, spontaneous movements, as an expression of neural activity, could be used as a marker for fetal brain status [3,54].
Based on all of these findings the following parameters were incorporated in the KANET [41]:
▪ Isolated head anteflexion. This movement is usually carried out slowly, but can also be fast and jerky. Activity of the f lexor muscles responsible for this pattern depends on the upper system from 34 gestational weeks. Abnormal movement looks abrupt when marked by sudden changes in subject and sharp transitions. Abnormally rhythmic movements are sometimes related to seizures occurring in utero. Absence of active flexion of the head in the 40th gestational week is one of the major neurological signs;
▪ Overlapping cranial sutures and head circumference. Normally cranial sutures are not overlapping. They are smooth, and ridges are not visible. Abnormal cranial ridges over suture or head circumference below normal limit are related to severe or moderate impairment of hemispheric growth;
▪ Isolated eye blinking (Figure 3). A reflex that closes and opens the eyes rapidly by involuntary, normal, periodic closing or by voluntary action. Movement looks fluent, smooth and unconstrained. The presence of this movement indicates absence of the CNS depression;
▪ Facial alteration (grimace or tongue expulsion) (Figure 4). The wrinkling of the brows or face in frowning, sometimes characterized by expulsion of the tongue. The presence of this movement indicated the absence of CNS depression. Almost absent mimic of the face or very rare movements (face looks always the same, mask-like face) is abnormal;

Figure 4.A sequence of images of the fetus recorded by 3D/4D sonography showing facial alterations, grimace or tongue expulsion. Reproduced with permission from [74]..

Figure 5.Image of the fetus recorded by 3D/4D sonography showing neurological sign of the thumb, the adduction of the thumb in a clenched fist. Reproduced with permission from [74].
▪ Mouth opening (yawning or mouthing). Yawning is characterized with prolonged wide opening of the jaws followed by quick closure, retroflexion of the head and elevation of the arms. Mouthing indicates that the fetus is opening the mouth. Sometimes consists of displacements of tongue and/or larynx. The presence of this movement indicates the absence of CNS depression. Absence of movements or very rare movements of the tongue and yawning are abnormal;
▪ Isolated hand and leg movements. Rapid or slow movements, can involve extension, flexion, external and internal rotation, or abduction and adduction of an extremity, without movements in other body parts. Automatic leg movement or walking movement is a precompetent stage, present very early in fetal life and still at birth, that diminishes in the first postnatal 3 months. Apparently, automatic walking movement disappears but is later involved in the automatization of independent walk for the rest of the life. This is a typical example of ‘change of power’ from a lower (brainstem) to a higher (cortical) command. Abnormal isolated hand and leg movement during prenatal life is characterized by poor repertoire when the sequence of successive components is monotonous and movements do not occur in the complex manner. Furthermore, the movement is characterized as cramped when it looks rigid, with lack of the normal smooth and fluent character. Abnormally rhythmic movements are sometimes related to seizures occurring in utero;
▪ Hand-to-face movements. The hand touches the face parts, sometimes with extension and flexion of the fingers. Abnormal movement looks abrupt when it is marked by sudden changes in subject and sharp transitions. Abnormally rhythmic movements are sometimes related to seizures occurring in utero;
▪ Finger movements and thumb position. Normally thumb is outside the fist most of the time, and finger movements are present (Figure 5). This motor activity depends on the lower system up to 30–32 gestational weeks and switches to the upper control later on. Neurological sign of the thumb, that indicates brain impairment, is demonstrated when the adduction of the thumb in a clenched fist is nonreducible. In addition, disturbance in fingers and thumb movements correlated with absence of spontaneous motor activity. Unilateral side of the clenched fist is a precious orientation in case of infarction of the middle cerebral artery;
▪ Gestalt perception of GMs. This parameter is defined as overall perception of the body and limb movements with their qualitative assessment (fluency, variability and amplitude). Normally movements are synchronized showing fluency and elegance, creating the impression of complexity and variability. Abnormal findings include poor amplitude, variability and fluency of the movements. The identification of the ‘CNS depression’ during fetal life is based on quality of GMs [41].
Assessment of disturbed fetal behavior using 2D & 4D ultrasound
Abnormalities in fetal motor activity may consist of a delayed first emergence of specific movements, quantitative changes, an abnormal quality of movements (i.e., changes in the execution of movements patterns) and an abnormal development of fetal behavioral (or sleep) states [57]. Abnormal movement patterns, indicative of altered brain or muscular development, have been described in fetuses from pregnancies complicated with various pathological factors [58]. Common features in all these cases are the qualitative changes in the execution of movement patterns, which are abrupt and forceful, with large amplitude in the majority of fetuses with a chromosomal or CNS defect and slow, with small amplitude, in the others [3,57].
Intrigued by fetal activity, the researchers studied the behavior of fetuses in various pathological conditions. The first study on diabetes-related inf luence on fetal motoric activity revealed delayed emergence of fetal behavioral patterns. The results showed that there is a delay of 1–2 weeks in almost all observed movement patterns emerging in the first 12 weeks of gestation. Only fetal breathinglike movements were observed for the first time at the same gestational age as in the control group [59]. Furthermore, fetal breathing-like movements in relation to other parameters of fetal wellbeing in the late diabetic pregnancies were studied. Results showed that breathing-like movements in late diabetic pregnancy were not influenced by Braxton Hicks’ contractions and did not showing a clear-cut state-dependency. It was concluded that the (neural) mechanism underlying fetal breathing-like movements differs from that in normal pregnancy [60].
Van Vliet et al. showed that the quality and quantity of the growth restricted fetal motility. Authors suggest that some aspects of the CNS function are disturbed in growth-retarded fetuses, even in the absence of fetal distress [61]. Results of another study were in accordance with previous findings that growth restricted fetuses show a delay in the integration of behavioral patterns and a lower coincidence of behavioral states. These findings are particularly evident in the fetuses with a severe increase of peripheral vascular resistance (absence of end diastolic flow in descending aorta) suggesting that a delay in the CNS development is present in asymmetrical growth-retarded fetuses and that there is a possible relationship of this delay to the degree of peripheral vascular resistance [62]. In addition, in fetuses suffering intrauterine growth restriction (IUGR), fetal movements become slower and monotonous, resembling cramps, and their variability in strength and amplitude is reduced. The alterations in amplitude and complexity of movements in these fetuses do not appear to be due to the oligohydramnios. In cases of premature rupture of fetal membranes and a subsequently reduced volume of amniotic f luid, movements occur less frequently, but their complexity resembles that of movements performed in the normal volume of amniotic fluid [63]. First study of fetal behavior using 4D ultrasound showed that the median value of all movement patterns in the normal fetuses differed from fetuses with IUGR [64]. Statistical evaluation revealed significant differences in the distribution of the movements between these groups. A tendency that IUGR fetuses have less behavioral activity than normal fetuses was noted in all observed movement patterns. Correlation reached statistical significance between normal and IUGR fetuses in the third trimester in handto- head, hand-to-face and head retroflexion.
These recent data on IUGR fetuses obtained by 4D sonography are stimulating and might result in a more effective strategy to assess development before birth and may encourage future use of 4D ultrasound for quantitative and qualitative assessment of fetal behavior as possible indicators of the neurological condition in IUGR fetuses.
Furthermore, severe reduction of fetal movements at the 27th week detected by prenatal 2D ultrasound was observed in the case of transplacental infection with coxsackie B3, confirmed by molecular techniques. Late onset of fetal akinesia deformation sequence with mild arthrogryposis was the finding at fetal autopsy following interruption of the pregnancy [65]. A study on the effect of Listeria monocytogenes on fetal motility showed that presentation of the infection includes premature labor, an influenzalike illness and reduced fetal movements [66]. Also, it was found that the breathing-like movements could be used as a predictor of intraamniotic infection [67].
Recently results regarding study of fetal GMs and echogenicity changes in the fetal brain were published [68]. The study included 121 fetuses from pregnancies affected by hypertensive disorders and/or preterm labour, at risk for preterm birth. Qualitative abnormal GMs were frequent in fetuses of compromised pregnancies, and correlate with hypertensive disorders and oligohydramnios. The amplitude of GMs was most frequently affected. Abnormal GMs relate to moderate echogenicity changes especially in the periventricular area of the fetal brain, while normal GMs predict absence of moderate echogenicity changes. This is the first study relating fetal GMs to echogenicity changes in the fetal brain [68].
To produce the new scoring test, the Zagreb group identified severely brain damaged infants and those with optimal neurological findings by comparing fetal with neonatal findings [41]. Ten fetuses who were postnatally (according to neurological assessment) described as mildly or moderately abnormal achieved a prenatal score of 5 to 13 , while another ten fetuses postnatally assigned as neurologically abnormal had a prenatal score from 0 to 5. Among this group four fetuses had alobar holoprosencephally, one had severe hypertensive hydrocephaly, one had tanatophoric dysplasia and four fetuses had multiple malformations. These preliminary results demonstrated ability of KANET to identify abnormal behavior in severely neurologically damaged fetuses.
To verify the new scoring test, study has been continued in several collaborative centers (Zagreb, Istanbul, Bucharest and Doha) [69]. This multicentric research included 228 fetuses from high-risk pregnancies, of whom 18 had a definite abnormal KANET score. Of these 18 pregnancies, five pregnancies were terminated, and six fetuses died in utero. Of seven fetuses with abnormal KANET score, postnatal neurological assessment by Amiel Tison’s method revealed three newborns out of seven fetuses to be abnormal (arthrogryposis, vermis aplasia and neonate of the mother with the previous child with CP), while four were considered normal (ventriculomegaly, preeclampsia, thrombophylia, oligohydramnios). The three very illustrative cases with abnormal KANET scoring were arthrogryposis, vermis aplasia, and the fetus whose previous sibling had verified cerebral palsy. The fetuses in these three cases had especially reduced facial movements, the faces were mask-like during repeated scans. Fetuses with vermis aplasia and arthrogryposis had normal cranial sutures but the isolated head flexion was small in range for both cases. Isolated hand movements, hand-to-face and leg movements were poor in repertoire for all three cases. The finger movements were cramped and invariable in all three cases. The Gestalt perception of GMs was also abnormal in these cases. In this study the behavior of a fetus with acranius was also longitudinally followed [69]. It has been observed that the fetus at 20 weeks of gestation had hypertonic movements with high amplitude and high speed. The movements emerged abruptly with burst-paused patterns, the variability of head movements was missing, without changes of facial expressions. As the gestational age advanced and the motor control was shifting from lower to upper control centers the movement patterns changed as well. At the gestational age of 32 weeks the fetus had no facial expressions (mask-like face) and hand movement repertoire was very poor. At 36 weeks the absence of both the facial expressions and limb movements was observed. In this fetus abnormal behavior patterns, as a result of lack of the appropriate control of the upper cortical centers on the motor activity, was clearly documented [69].
Another study conf irmed statistically significant difference in fetal behavioral patterns between the fetuses from low-risk and highrisk pregnancies [70]. Statistically significant difference for eight out of ten parameters of KANET has been demonstrated: isolated anteflection of the head, eye blinking, facial expressions (grimacing, tongue expulsion), mouth movements (mouthing, jawing, swallowing), isolated hand movement, hand-toface movement, fist and finger movements, and GMs. Authors have also confirmed statistically significant, moderate correlation of KANET and ATNAT tests. In a practical sense, this means that the neuropediatricians who examined the newborns with ATNAT test confirmed the results of KANET [70].
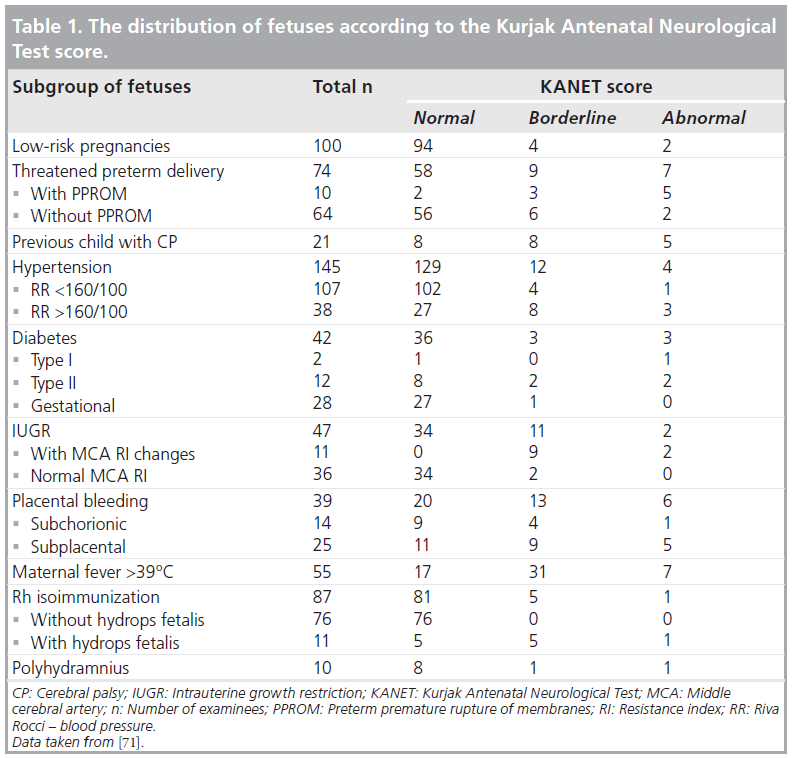
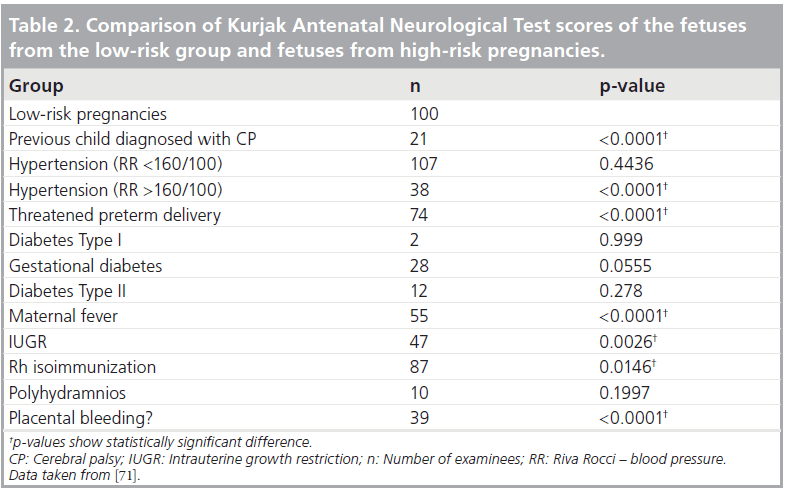
New results regarding the potential of 4D sonography in the assessment of fetal behavior in high-risk pregnancies were recently published [71]. The group in Khartoum applied KANET to a large number of fetuses during the period of 1 year. The aim of the study was to assess the behavior in a large sample of fetuses from normal and high-risk pregnancies by application of the KANET scoring test and to compare the scores obtained in low- and highrisk pregnancies (Tables 1 & 2). In this prospective longitudinal cohort study, the KANET was applied in 620 singleton pregnancies, between the 26th and 38th week of gestation. There were 520 pregnant women in the high-risk and 100 pregnant women in the low-risk group. Contrary to the previous studies, the fetuses with congenital anomalies and multiple pregnancies were excluded from the study. The high-risk group of patients consisted of the following subgroups: threatened preterm delivery with or without preterm premature rupture of membranes (PPROM), previous child diagnosed with CP, hypertension in pregnancy with or without preeclampsia, diabetes before pregnancy or gestational diabetes, IUGR, polyhydramnios, Rh isoimmunization, placental bleeding, and maternal fever above 39°C. Fetal KANET scores from low-risk and high-risk pregnancies were compared, and the difference was statistically significant. A statistically significant difference was found between KANET scores of the fetuses from the low-risk group compared with the following subgroups of the high-risk group: previous child diagnosed with CP, hypertension (RR >160/100), threatened preterm delivery, maternal fever, IUGR, Rh isoimmunization, placental bleeding. Furthermore, KANET scores signif icantly differed comparing threatened preterm delivery with PPROM versus threatened preterm delivery without PPROM; hypertension above 160/100 mmHg versus hypertension below 160/100 mmHg; diabetes before pregnancy versus gestational diabetes; IUGR with decreased resistance index of middle cerebral artery versus IUGR without decreased resistance index of middle cerebral artery; and Rh isoimmunization without hydrops fetalis versus Rh isoimmunization with hydrops fetalis. Among the fetuses with abnormal KANET score, the most frequently presented were fetuses from the threatened preterm delivery group. Comparison of individual KANET parameters between the fetuses from the low-risk and highrisk pregnancies showed statistically significant difference for overlapping cranial sutures and head circumference, isolated eye blinking, facial expressions (grimacing and tongue expulsion), mouth movements (yawning and mouthing), isolated hand movements, isolated leg movements, hand to face movement, finger movements, and GM. For isolated head anteflexion, the difference was not statistically significant [71]. Up to now, this was the study with the largest number of fetuses where prenatal KANET test was applied.
Furthermore, in a recently published case report KANET indicated normal early neurological development of the child, confirmed by postnatal tests, despite unfavorable intrauterine conditions, diagnosed IUGR and fetal hypoxemia [72].
Preliminary results have confirmed the usefulness of KANET in fetal behavior assessment. The KANET test has the potential to detect and discriminate normal from borderline and abnormal fetal behavior in normal and in high-risk pregnancies, which means that it could become a valuable diagnostic tool for fetal neurological assessment [41,69–75]. However, further studies in a large population are required before recommending the use of the test in routine clinical practice. In addition, it seems necessary to simplify the test, maybe by grouping some of the parameters, making it more applicable as the screening tool for prenatal neurological assessment. Furthermore, sensitivity, specificity, negative and positive predictive value, intraobserver and interobserver reproducibility should also be investigated. KANET is the first prenatal neurological screening test based on the 4D ultrasound technique, whose preliminary results are promising [41,69–75]. Nevertheless, its value in the assessment of integrity of the fetal CNS needs to be confirmed by studies that are in progress in several world university centers.
Conclusion
The use of 4D imaging in the behavioral assessment of fetuses enabled a better evaluation of fetal motoric patterns, especially of the qualitative features of movements and fetal face movements. The new scoring system for fetal behavior, KANET, is based on 4D ultrasound. Preliminary results of this prenatal neurological screening test are promising. However, its value is yet to be estimated in the studies including large numbers of fetuses and by long-term neurological follow-up of children from these pregnancies.
Future perspective
4D ultrasound could become a valuable tool in the neurological assessment of fetus. It could also facilitate the evaluation of interhuman contact in twin pregnancies in utero. This novel technique may assist in the evaluation of fetal behavior and intertwin contact, and offer potential advantages relative to conventional 2D ultrasound. 4D ultrasound should become an important modality in future research on fetal neurobehavioral development and the prenatal identification of severely brain-damaged infants. Further studies involving a larger sample size are needed to ascertain the role of 4D ultrasound in the evaluation of fetal neurobehavioral development.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Papers of special note have been highlighted as: * of interest
References
- Nijhuis JG. Neurobehavioral development of the fetal brain. In: Fetal Behaviour: Developmental and Perinatal Aspects. Nijhuis JG (Ed.). Oxford University Press, Oxford, UK, 489 (1992).
- Nijhuis JG. Fetal behavior. Neurobiol. Aging 24, 41–46 (2003).
- Prechtl HF. Qualitative changes of spontaneous movements in fetus and preterm infant are a marker of neurological dysfunction. Early Hum. Dev. 23(3), 151–158 (1990).
- Timor-Tritsch IE, Platt LD. Threedimensional ultrasound experience in obstetrics. Curr. Opin. Obstet. Gynecol. 14(6), 569–575 (2002).
- Kossoff G. Basic physics and imaging characteristics of ultrasound. World J. Surg. 24(2), 134–142 (2000).
- Lee A. Four-dimensional ultrasound in prenatal diagnosis: leading edge in imaging technology. Ultrasound Rev. Obstet. Gynecol. 1, 194–198 (2001).
- Kozuma S, Baba K, Okai T, Taketani Y. Dynamic observation of the fetal face by three-dimensional ultrasound. Ultrasound Obstet. Gynecol. 13(4), 283–284 (1999).
- Campbell S. 4D or not 4D: that is the question. Ultrasound Obstet. Gynecol. 19, 1–4 (2002).
- Kurjak A, Azumendi G, Andonotopo W, Salihagic-Kadic A. Three- and fourdimensional ultrasonography for the structural and functional evaluation of the fetal face. Am. J. Obstet. Gynecol. 196(1), 16–28 (2007).
- Kurjak A, Azumendi G, Vecek N et al. Fetal hand movements and facial expression in normal pregnancy studied by fourdimensional sonography. J. Perinat. Med. 31(6), 496–508 (2003).
- Andonotopo W, Stanojevic M, Kurjak A, Azumendi G, Carrera JM. Assessment of fetal behavior and general movements by fourdimensional sonography. Ultrasound Rev. Obstet. Gynecol. 4, 103–114 (2004).
- Kurjak A, Pooh RK, Merce LT, Carrera JM, Salihagic-Kadic A, Andonotopo W. Structural and functional early human development assessed by three-dimensional and fourdimensional sonography. Fertil. Steril. 84(5), 1285–1299 (2005).
- de Vries JIP, Visser GH, Prechtl HF. The emergence of fetal behavior, I. Qualitative aspect. Early Hum. Dev. 7, 301–322 (1982).
- Salihagic Kadic A, Predojevic M, Kurjak A. Advances in fetal neurophysology. In: Fetal Neurology. Pooh RK, Kurjak A (Eds). Jaypee Brothers Medical Publishers, New Delhi, India, 161–221 (2009).
- Andonotopo W, Kurjak A, Azumendi G. Ultrasound studies on early pregnancy. In: Atlas of Clinical Application of Ultrasound in Obstetrics and Gynecology. Kurjak A, Carrera JM (Eds). Jaypee Brothers Medical Publishers, New Delhi, India (2005).
- Azumendi G, Arenas JB, Andonotopo W, Kurjak A. Three dimensional sonoembriology. In: Textbook of Transvaginal Sonography. Kurjak A, Arenas JB (Eds). Taylor & Francis, London, UK, 407 (2005).
- Andonotopo W, Medic M, Salihagic-Kadic A, Milenkovic D, Maiz N, Scazzocchio E. The assessment of fetal behavior in early pregnancy: comparison between 2D and 4D sonographic scanning. J. Perinat. Med. 33(5), 406–414 (2005).
- Hopkins B, Prechtl HFR. A qualitative approach to the development of movements during early infancy. In: Continuity of Neural Functions from Perinatal to Postnatal Life. Prechtl HFR (Ed.). Blackwell Scientific Publications, Oxford, UK, 179–197 (1984).
- Prechtl HF. Qualitative changes of spontaneous movements in fetus and preterm infant are a marker of neurological dysfunction. Early Hum. Dev. 23(3), 151–158 (1990).
- Kurjak A, Vecek N, Hafner T, Bozek T, Funduk-Kurjak B, Ujevic B. Prenatal diagnosis: what does four-dimensional ultrasound add? J. Perinat. Med. 30(1), 57–62 (2002).
- Kurjak A, Vecek N, Kupesic S, Azumendi G, Solak M. Four dimensional ultrasound: how much does it improve perinatal practice? In: Controversies in Perinatal Medicine. Studies on the Fetus as a Patient. Carrera JM, Chervenak FA, Kurjak A (Eds). Parthenon Publishing, NY, USA 222 (2003).
- Kurjak A, Stanojevic M, Andonotopo W, Salihagic-Kadic A, Carrera JM, Azumendi G. Behavioral pattern continuity from prenatal to postnatal life – a study by four-dimensional (4D) ultrasonography. J. Perinat. Med. 32(4), 346–353 (2004). & Demonstrates that there is a continuity from fetal to neonatal behavior, especially in terms of facial movements and hand movements directed to other parts of the face.
- Pooh RK, Ogura T. Normal and abnormal fetal hand positioning and movement in early pregnancy detected by three and fourdimensional ultrasound. Ultrasound Rev. Obstet. Gynecol. 4, 46–51 (2004).
- Kurjak A, Andonotopo W, Hafner T et al. Normal standards for fetal neurobehavioral developments – longitudinal quantification by four-dimensional sonography. J. Perinat. Med. 34(1), 56–65 (2006). & In this study normal standards for fetal neurobehavioral development using longitudinal observations through all trimesters by 4D sonography have been constructed.
- Hata T, Kanenishi K, Sasaki M. Fourdimensional sonographic assessment of fetal movement in the late first trimester. Int. J. Gynfalse-positivecol. Obstet. 109(3), 190–193 (2010).
- Hata T, Dai SY, Marumo G. Ultrasound for evaluation of fetal neurobehavioral development: from 2D to 4D ultrasound. Infant Child Dev. 19(1), 99–118 (2010).
- Kuno A, Akiyama M, Yamashiro C, Tanaka H, Yanagihara T, Hata T. Threedimensional sonographic assessment of fetal behavior in the early second trimester of pregnancy. J. Ultrasound Med. 20(12), 1271–1275 (2001).
- Awoust J, Levi S. Neurological maturation of the human fetus. Ultrasound Med. Biol. (Suppl. 2), 583–587 (1983).
- Inoue M, Koyanagi T, Nakahara H. Functional development of human eyemovement in utero assessed quantitatively with real-time ultrasound. Am. J. Obstet. Gynecol. 155, 170–174 (1986).
- de Vries JIP, Visser GHA, Mulder EJH, Prechtl HFR. Diurnal and other variations in fetal movement and heart rate patterns at 20–22 weeks. Early Hum. Dev. 15(6), 333–348 (1987).
- D’Elia A, Pighetti M, Moccia G, Santangelo N. Spontaneous motor activity in normal fetus. Early Hum. Dev. 65(2) 139–144 (2001).
- Natale R, Nasello-Paterson C, Turlink R. Longitudinal measurements of fetal breathing, body movements, and heart rate accelerations, and decelerations at 24 and 32 weeks of gestation. Am. J. Obstet. Gynecol. 151, 256–263 (1985).
- Eller DP, Stramm SL, Newman RB. The effect of maternal intravenous glucose administration on fetal activity. Am. J. Obstet. Gynecol. 167, 1071–1074 (1992).
- Haddres-Algra M. Putative neural substrate of normal and abnormal general movements. Neurosci. Biobehav. Rev. 31(8), 1181–1190 (2007).
- Yan F, Dai SY, Akther N, Kuno A, Yanagihara T, Hata T. Four-dimensional sonographic assessment of fetal facial expression early in the third trimester. Int. J. Gynaecol. Obstet. 94(2), 108–113 (2006).
- Visser GHA, Mulder EJH, Prechtl HFR. Studies on developmental neurology in the human fetus. Dev. Pharmacol. Ther. 18, 175–183 (1992).
- Mulder EJH, Visser GHA, Bekedan DJ, Prechtl HFR. Emergence of behavioural states in fetuses of Type-1 diabetic women. Early Hum. Dev. 15, 231–251 (1987).
- Hata T, Kanenshi K, Tanaka H, Marumo G, Sasaki M. Four-dimensional ultrasound evaluation of fetal neurobehavioral development. Donald School J. Ultrasound Obstet. Gynecol. 4(3), 233–248 (2010).
- Kurjak A, Miskovic B, Andonotopo W, Stanojevic M, Azumendi G, Vrcic H. How useful is 3D and 4D ultrasound in perinatal medicine? J. Perinat. Med. 35, 10–27 (2007).
- Pooh RK, Kurjak A. Fetal Neurology. Jaypee Brothers Medical Publishers, New Delhi, India (2009).
- Kurjak A, Miskovic B, Stanojevic M et al. New scoring system for fetal neurobehavior assessed by three- and four-dimensional sonography. J. Perinat. Med. 36, 73–81 (2008). & In the study a new scoring system for fetal neurobehavior based on prenatal assessment by 3D/4D sonography is proposed and described.
- Yigiter AB, Kavak ZN. Normal standards of fetal behavior assessed by four-dimensional sonography. J. Matern. Fetal Neonatal Med. 19, 707–721 (2006).
- Hadders-Algra M. General movements: a window for early, identification of children at high-risk of developmental disorders. J. Pediatr. 145, S12–S18 (2004).
- Gosselin J, Gahagan S, Amiel-Tison C. The Amiel-Tison neurological assessment at termconceptual and methodological continuity in the course of follow up. Ment. Retard. Dev. Disabil. Res. Rev. 11, 34–51 (2005).
- Amiel-Tison A, Gosselin J, Kurjak A. Neurosonography in the second half of fetal life a: neonatologists point of view. J. Perinat. Med. 34, 437–446 (2006).
- Amiel-Tison C. Neurological assessment of the neonate revisiteda personal view. Dev. Med. Child Neurol. 32, 1109–1113 (1990).
- Amiel-Tison C, Gosselin J. Neurological Development from Birth to Six Years. Johns Hopkins University Press, Baltimore, MA, USA (2001).
- Amiel-Tison C. Update of the Amiel-Tison Neurological assessment for the term neonate or at 4 weeks corrected age. Pediatr. Neurol. 27, 196–212 (2002).
- Amiel-Tison C, Gosselin J. From neonatal to fetal neurology: some clues for interpreting fetal findings. In: Fetal Neurology. Pooh RK, Kurjak A (Eds). Jaypee Brothers Medical Publishers, New Delhi, India (2009).
- Kurjak A, Pooh RK, Tikvica A et al. Assessment of fetal neurobehavior by 3D/4D ultrasound. In: Fetal Neurology. Pooh RK, Kurjak A (Eds). Jaypee Brothers Medical Publishers, New Delhi, India, 221–287 (2009).
- Hadders-Algra M. General movement during prenatal and early postnatal life. In: The Fetus in Three Dimensions: Imaging, Embryology, and Fetoscopy. Kurjak A, Azumendi G (Eds). Informa Health Care, London, UK (2007).
- Cioni G, Prechtl HFR, Ferrari F, Paolicelli PB, Einspieler C, Roversi MF. Which better predicts later outcome in full term infants quality of general movements or neurological examination? Early Hum. Dev. 50, 71–85 (1997).
- Ferrari F, Cioni G, Prechtl HFR. Qualitative changes of general movements in preterm infants with brain lesions. Early Hum. Dev. 23, 193–233 (1990).
- Einspieler C, Prechtl HFR. Prechtls assessment of general movements. A diagnostic tool for the functional assessment of the young nervous system. Ment. Retard. Dev. Disabil. Res. Rev. 11, 61–67 (2005).
- Einspieler C, Prechtl HFR, Bos AF, Ferrari F, Cioni G. Prechtls Method on the Qualitative Assessment of General Movements in Preterm, Term and Young Infants. Mac Keith Press, Cambridge, UK (2004).
- Hadders-Algra M, Klip Van den Niewcendijk WJ, Martijn A, van Eyken L. Assessment of general movementstowards a better understanding of a sensitive method to evaluate brain function in young infants. Dev. Med. Child Neurol. 39, 89–89 (1997).
- Visser GH, Mulder EJ, Tessa Ververs FF. Fetal behavioral teratology. J. Matern. Fetal Neonatal Med. 23(Suppl. 3), 14–16 (2010).
- Visser GHA, Mulder EJH. Fetal movement patterns and fetal behavioural states. In: Ultrasound in Obstetrics and Gynaecology. Wladimiroff JW, Eik-Nes S (Eds). Elsevier, Philadelphia, PA, USA, 271–284 (2009).
- Visser GH, Bekedam DJ, Mulder EJ, van Ballegooie E. Delayed emergence of fetal behaviour in type-1 diabetic women. Early Hum. Dev. 12(2), 167–172 (1985).
- Mulder EJ, Leiblum DM, Visser GH. Fetal breathing movements in late diabetic pregnancy: relationship to fetal heart rate patterns and Braxton Hicks’ contractions. Early Hum. Dev. 43(3), 225–232 (1995).
- Van Vliet MA, Martin CB Jr, Nijhaus JG, Prechtl HF. Behavioural states in growthretarded human fetuses. Early Hum. Dev. 12, 183–197 (1985).
- Rizzo G, Arduini D, Pennestri F, Romanini C, Mancuso S. Fetal behaviour in growth retardation: its relationship to fetal blood flow. Prenat. Diagn. 7(4), 229–238 (1987).
- Sival DA, Visser GH, Prechtl HF. The relationship between the quantity and quality of prenatal movements in pregnancies complicated by intra-uterine growth retardation and premature rupture of the membranes. Early Hum. Dev. 30(3), 193–209 (1992).
- Andonotopo W, Kurjak A. The assessment of fetal behavior of growth restricted fetuses by 4D sonography. J. Perinat. Med. 34, 471–478 (2006).
- Konstantinidou A, Anninos H, Spanakis N et al. Transplacental infection of Coxsackievirus B3 pathological findings in the fetus. J. Med. Virol. 79(6), 754–757 (2007).
- Craig S, Permezel M, Doyle L, Mildenhall L, Garland S. Perinatal infection with Listeria monocytogenes. Aust. NZ J. Obstet. Gynaecol. 36(3), 286–290 (1996).
- Goldstein I, Romero R, Merrill S et al. Fetal body and breathing movements as predictors of intraamniotic infection in preterm premature rupture of membranes Am. J. Obstet. Gynecol. 159(2), 363–368 (1988).
- Rosier-van Dunné FM, van Wezel-Meijler G, Bakker MP, Odendaal HJ, de Vries JI. Fetal general movements and brain sonography in a population at risk for preterm birth Early Hum. Dev. 86, 107–111 (2010).
- Kurjak A, Abo-Yaqoub S, Stanojevic M et al. The potential of 4D sonography in the assessment of fetal neurobehavior – multicentric study in highrisk pregnancies. J. Perinat. Med. 38, 77–82 (2010).
- Miškovic B, Vasilj O, Stanojevic M, Ivankovic D, Kerner M, Tikvica A. The comparison of fetal behavior in high-risk and normal pregnancies assessed by four dimensional ultrasound. J. Matern. Fetal Neonatal Med. 23(12), 1461–1467 (2010).
- Talic A, Kurjak A, Ahmed B et al. The potential of 4D sonography in the assessment of fetal behavior in high-risk pregnancies. J. Matern. Fetal Neonatal Med. 24(7), 948–954 (2010)
- Predojevic M, Stanojevic M, Vasilj O, Kadic AS. Prenatal and postnatal neurological evaluation of a fetus and newborn from pregnancy complicated with IUGR and fetal hypoxemia. J. Matern. Fetal Neonatal Med. 24(5), 764–767. (2010).
- Kurjak A, Ahmed B, Abo-Yaguab S et al. An attempt to introduce neurological test for fetus-based on 3D and 4D sonography. Donald School Journal of Ultrasound Obstet. Gynecol. 2, 29–44 (2008).
- Kurjak A, Tikvica Luetic A, Stanojevic M et al. Further experience in the clinical assessment of fetal neurobehavior. Donald School Journal of Ultrasound in Obstetrics and Gynecology 4, 59–71 (2010).
- Kurjak A, Ahmed B, Miskovic B, Predojevic M, Salihagic Kadic A. Fetal behavior assessed by 4D sonography. In: Donald School Textbook of Ultrasound in Obstetrics and Gynecology (3rd Edition). Kurjak A, Chervenak FA (Eds). Jaypee Brothers Medical Publishers, New Delhi, India (In Press).


